

Background: Hodgkin Lymphoma (HL) Reed Sternberg cells express tumor associated antigens (TAA) that are potential targets for cellular therapies. We recently demonstrated that TAA specific T cells (TAA-T) targeting WT1, PRAME and Survivin were safe and associated with prolonged time to progression in solid tumors (Hont JCO 2019). Hence, we evaluated whether TAA-T cells are safe and elicit anti-tumor effects in patients with relapsed/refractory (rel/ref) HL. We further evaluated the safety of Nivolumab following the TAA-T infusion and its effect on the persistence of the TAA-T cells in vivo.
Methods: TAA-T products were generated from patients or healthy donors on 2 trials (NCT02203903; NCT03843294). Thirteen patients underwent procurement for product generation and 10 patients (2 allogeneic; 8 autologous) were infused TAA-T for rel/ref HL or as consolidation after autologous hematopoietic stem cell transplant (HSCT) at cumulative doses ranging from 0.5 X107 to 4 X107cells/m2. Patients were monitored for six weeks for safety and for response until disease progression. Seven patients received Nivolumab starting at 8 weeks after the first TAA-T infusion until disease progression or unacceptable toxicity.
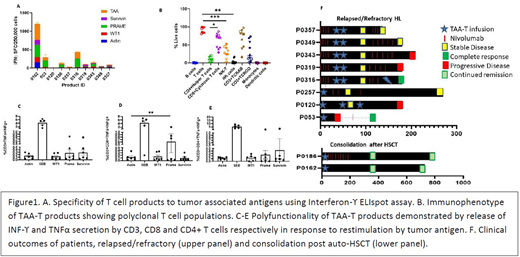
Results: TAA-T products (n=10) were polyclonal CD3+ T cells (Median 97%; 80.9-99.5%), comprised predominantly of CD4+ helper T cells (Median 10.5%; 1.74-20%) and CD8+ cytotoxic T cells (Median 70%; 29.3-87.5%). Specificity of TAA-T products was tested using Interferon-ϒ(INFϒ)-enzyme-linked immunospot (ELIspot) assay and defined as ≥ 2x spot-forming cells (SFC)/2.5X105cells against the tumor antigen as compared to irrelevant control antigen Actin(Figure 1). The median TAA specificity of the products was 2 antigens (range 0-3). All products were polyfunctional secreting INF-ϒ and TNF-α upon restimulation with tumor antigens (Fig 1).
Median age of patients was 36yrs (range16-53). Patients had received a median 6 lines of therapy including HSCT prior to receiving TAA-T. Median follow-up post TAA-T#1 was 6 months (range 32 days-2.5yrs). There were no dose limiting toxicities observed within the 6 week safety monitoring period. In patients receiving Nivolumab post TAA-T, there were no increased immune related events over expected. One patient had Grade 3 seizures, possibly related to Nivolumab, 2 patients developed hypothyroidism requiring thyroid supplements and one patient developed myositis and discontinued Nivolumab after 5 months. The 2 patients who received TAA-T (1 donor derived and one autologous) as consolidation post HSCT achieved a continued complete remission (CCR) for 2+ years. Of the 8 patients with rel/ref HL at the time of infusion, 1 had disease progression at 6 weeks. He then received Nivolumab off protocol and achieved complete remission (CR) but developed Grade 4 GVHD. The remaining 7 patients had stable disease (SD) at 6 weeks. At a median follow-up of 6 months (32 days-2.5 years), 1 patient had progressive disease(PD) at 3 months, 1 patient had a complete metabolic response at 6 months and proceeded to allogeneic HSCT for definitive cure. 2 patients had PD at 6 months and the other 2 patients continue with SD at 6 months and remain on Nivolumab (Fig 1).
All patients with objective responses (stable disease or better) recovered functional TAA-T cells in the peripheral blood at 3 months as detected by anti-Interferon-ϒ ELISPOT and reported as mean SFC/1 X105 cells for WT1(14±SD18.1); PRAME (17.4±15.3) and Survivin (4.5±7) compared to those with progressive disease with mean SFC/1 X105 cells for WT1 1.4(±2.3); PRAME (6.7±15.5) and Survivin (0.8±1.2). To evaluate TAA-T persistence, unique T cell receptor clonotypes defined in the TAA-T product and not present at baseline were detected in the peripheral blood 6 weeks post TAA-T, long-term persistence data and evaluating the effect on the TCR repertoire when adding nivolumab are pending.
Conclusion: TAA-T cells given in combination with Nivolumab were safe when administered to patients with rel/ref HL with prolonged clinical responses (ranging from SD to CCR) observed in multiply relapsed patients.
Glenn:Genentech: Research Funding. Hanley:Mana Therapeutics: Honoraria, Other: Board Member; Cellevolve: Honoraria, Other: Board(Scientific Advisory Board). Bollard:Mana Therapeutics: Other: IP.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal